|
|
Cecal Volvulus
General Considerations
- Volvulus is 3rd most common cause of colonic obstruction
- Following obstructing carcinoma and inflammatory stricture
- Two most common forms are
- Cecal volvulus can be associated with
- Abnormally long mesentery of cecum and ascending colon
- Leads to mobility of right colon predisposing to volvulus
- Other factors must be at play, though, since 10% of population has such a long mesentery yet few develop cecal volvulus
- Cecal volvulus has been associated with obstructing lesions of the left colon from carcinoma or diverticulitis
- Ascending colon twists on its longitudinal axis from 180° to 360° and rotates cecum upward and to left of midline
- Age peak: 20-40 years; M > F
Clinical Findings
- Patients present most often with an acute abdomen
- Colicky abdominal pain of sudden onset
- Most cases of cecal volvulus reportedly occur in patients while they are asleep with normal side to side movement during sleep possibly resulting in displacement of the right colon to an abnormal location
- Diagnosis is usually by plain film appearance
Imaging Findings
- Markedly dilated cecum
- "Kidney-shaped" distended cecum
- Usually positioned in LUQ or to the left of the midline
- Most obstructions are complete so there is little gas in the rest of the colon
- If barium enema is done, tapered end of barium column points toward torsion
- Beak configuration to end of barium column
- About 10-33% of cecal volvuli are cecal bascules
- Cecum does not rotate around its luminal axis
- Consistent feature of cecal bascule is presence of a constricting band across the ascending colon, the origin of which is not certain
- Cecum folds anteromedial to the ascending colon
- Produces a flap-valve occlusion at the site of flexion
- Occurs in a transverse plane and is associated with marked distension of the cecum
- Often displaced into the center of the abdomen
- Findings
- Distended air-filled cecum is located more centrally
Treatment
- Reduction using barium in an enema may be tried
- Treatment is usually surgical
Complications
- Closed-loop obstruction that can lead to
Prognosis
- Mortality between 20-40% in elderly


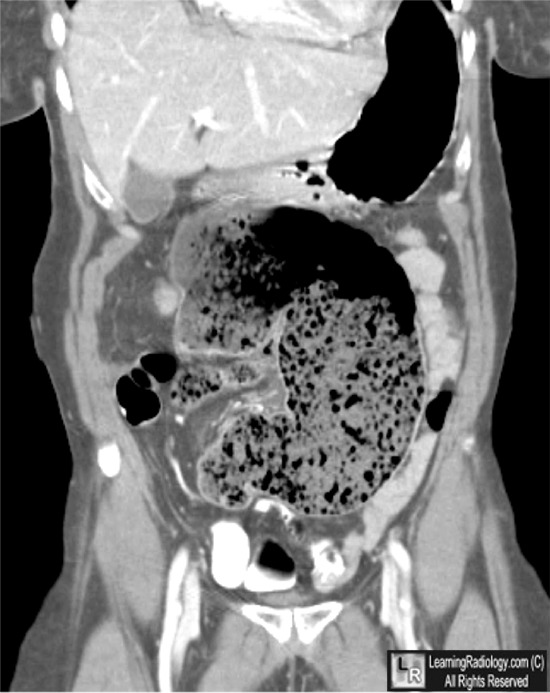
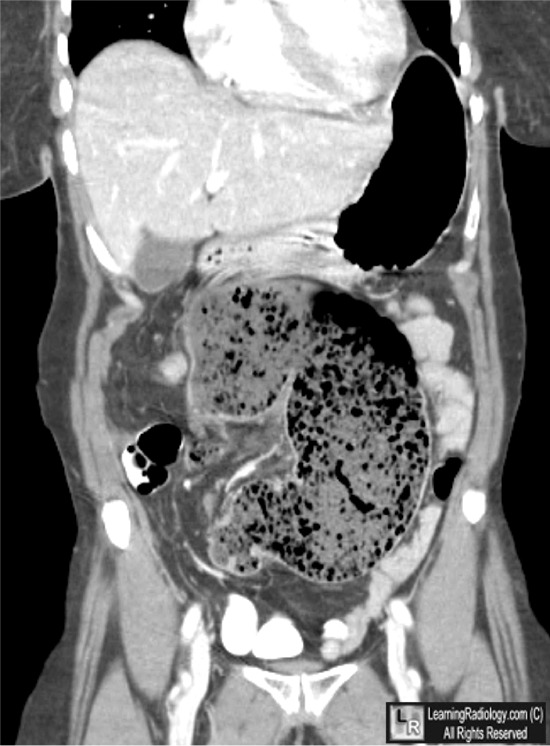
Cecal Volvulus. Two coronal reformatted CT scans of the abdomen are shown.
In the upper photo, the white arrows point to the region of the twist in the cecum (C) itself. In the lower photo, the white arrow indicates the cecum (C) flips from the right lower quadrant
to the left upper quadrant, rotating on its mesentery.
For these same photos without the arrows, click here and here
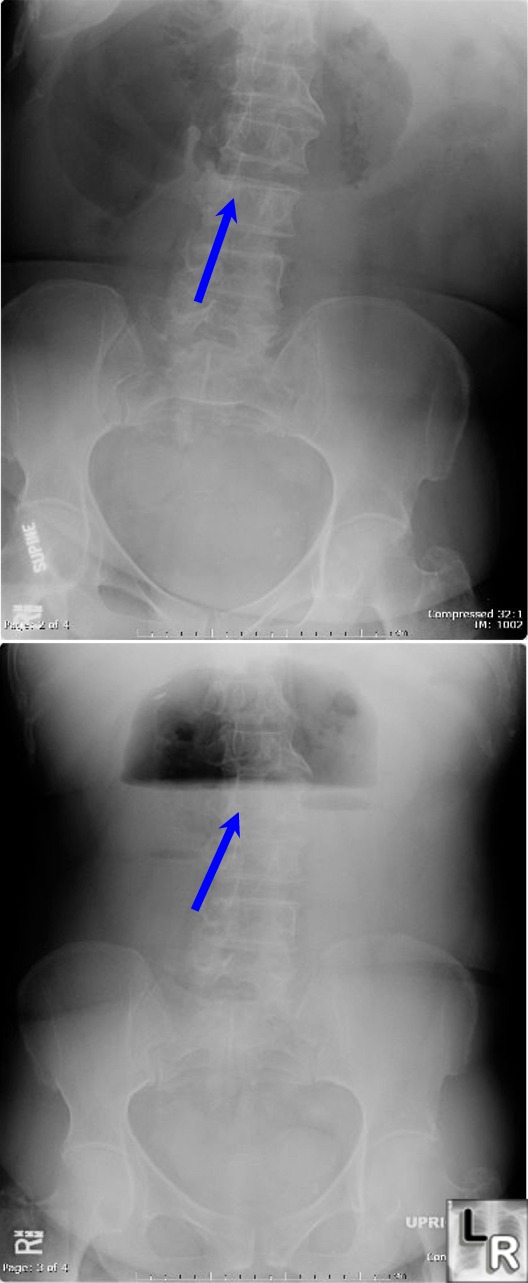
Cecal Volvulus. Two radiographs of the abdomen, the upper supine and the lower erect, show a markedly dilated loop of large bowel (blue arrow) with a smooth, tapered end that appears to be the cecum. There is no gas in the large bowel distal to the dilated cecum.
For more information, click on the link if you see this icon 
Ali Nawaz Khan and John Howat; eMedicine, Cecal Volvulus
Halpert and Feczko: The Requisites, 2nd ED, Gastrointestinal Radiology
|
|
|

{kind=link}
{kind=link}