|
|
Postpericardiotomy Syndrome
Dressler’s Syndrome/Postmyocardial Infarction Syndrome/
Postcardiac Injury Syndrome
General Considerations
- Autoimmune and febrile illness that can follow coronary artery bypass surgery
- May also be seen following myocardial infarction (Dressler’s syndrome)
- Reported to occur in 10-40% of cases
- Combination of pericarditis, pleuritis and pneumonitis
- Believed to have immunologic cause
- Possibly a latent viral infection may be involved in cause
Clinical Findings
- Symptoms typically appear 2-3 weeks following infarct/surgery–sometimes years
- May last for weeks or months
- Pleuritic chest pain (91%)
- Fever
- Pericardial and pleural effusion
- Pericardial friction rub
- Effusions can be bloody and cause tamponade
- Also rales
- Shortness of breath
- Leukocytosis
Imaging Findings
- Diagnosis can usually be made from a combination of the clinical picture and chest radiographs (95% abnormal)
- Cardiac silhouette enlargement from pericardial effusion and mild to moderate-sized left (usually) pleural effusion
- Pleural effusion may be bilateral
- Pleural effusions (83%)
- Parenchymal opacities (74%)
- Enlarged cardiac silhouette from pericardial effusion (49%)
Differential Diagnosis
- Different from more common post myocardial infarction reactive changes
- Occurs between days 2 and 4 after the infarction
- Congestive heart failure
- Pneumonia
- Reaction to medication
Treatment
- High dose aspirin
- Steroids

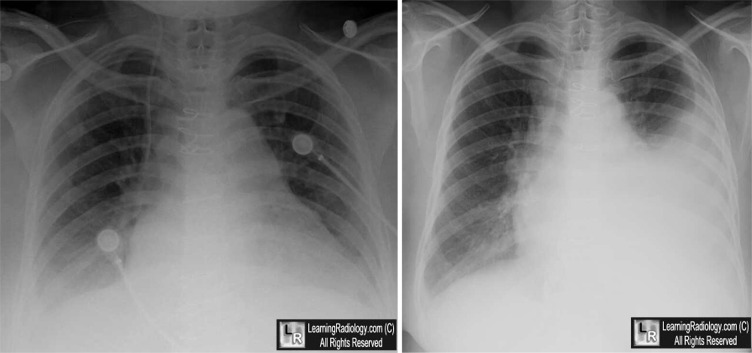
Postpericardiotomy Syndrome. Left: Immediately after coronary artery jump graft surgery, there are small bilateral effusions. Right:Three weeks later, there is a moderately large left pleural effusion (white arrow). There are no other signs of congestive heart failure.
For these same photos without the arrows, click here
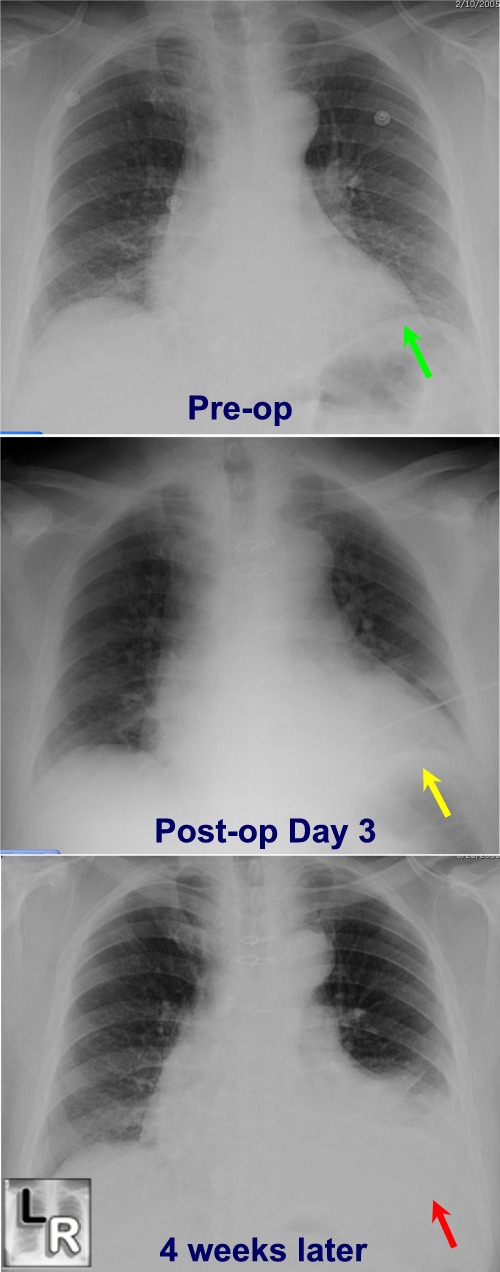
Three sequential images of the chest show a
pre-op chest in which the left lung base is clear (green
arrow);
on the third day post-op coronary artery jump bypass surgery,
there is subsegmental atelectasis
at the left base (yellow arrow);
Four weeks later, there is a left pleural effusion and
subsegmental atelectasis visible (red arrow)
For more information, click on the link if you see this icon 
|
|
|

{kind=link}