|
|
Discitis
General Considerations
- Usually the result of blood–borne agents
- Especially from lung and urinary tract
- Average age of onset is in children around 6 years
- Most common pathogen is staphylococcus
- Also Streptococcus
- Gram-negative rods in IV drug abusers or immunocompromised patients
- E. Coli
- Proteus
- Non-pyogenic
- Tuberculosis
- Coccidioidomycosis
- May occur as a result of invasive procedure
- Surgery
- Discography
- Myelography
Pathogenesis
- In children, probably begins in still vascularized disc
- In adults, in anterior inferior corner of vertebral body with spread across disk to adjacent vertebral endplate
Site of involvement
- L3/4
- L4/5
- Unusual above T9
- Usually involvement of one disk space (occasionally 2)
- Bacteria destroy disk and both contiguous end-plates
Imaging Findings
- Conventional Radiography
- Narrowing and destruction of an intervertebral disk
- Earliest plain film sign
- Indistinctness of adjacent endplates with destruction
- Often associated with bony sclerosis of the two contiguous vertebral bodies
- Paravertebral soft tissue mass
- Endplate sclerosis (during healing phase beginning anywhere from 8 weeks to 8 months after onset)
- Bone fusion after 6 months to 2 years
- MRI
- Decreased marrow intensity on T1-weighted images in two contiguous vertebrae
- High signal intensity on T2
- Because of associated edema
- Disk space and paravertebral soft tissues enhance on MRI
Clinical
- Pain is present if disease is acute
- Point tenderness
- Malaise
- Irritability in children
- Referred hip pain
- Inability to bear weight
- Course of discitis is frequently more benign in children than adults
- Disk space is narrowed but no destruction of contiguous vertebral bodies
- Osteomyelitis of the vertebral body
- Usually the result of discitis
- But can occur from direct involvement from hematogenous dissemination to body
- MRI findings are similar to discitis
- Bone scan will be positive
- Gallium scan or Indium-111 scan will be positive
- Renal spondyloarthropathy
- May resemble discitis
- Usually involves cervical spine
- Destruction of disk space and adjacent vertebral bodies
- Signal on T2 is low rather than high
- No clinical evidence of infection
Complications
Treatment
- Bone fusion after 6 months to 2 years
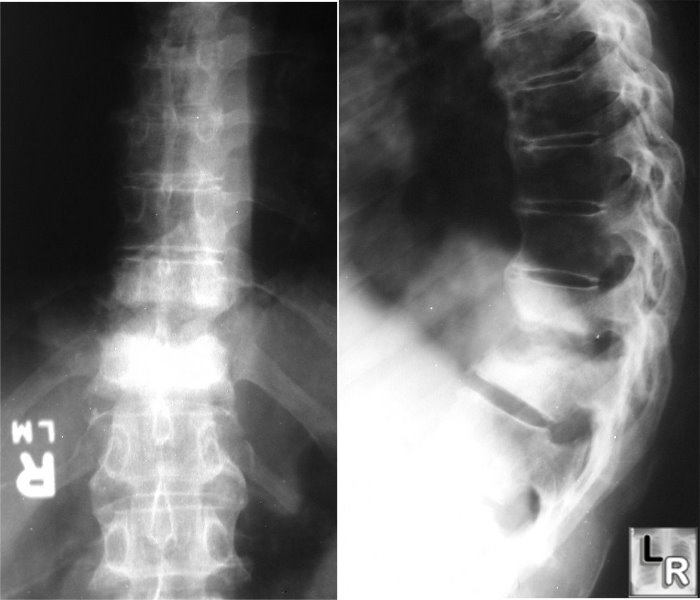
Discitis, Thoracic Spine. Frontal and lateral radiographs of the thoracic spine demonstrate destruction of the endplates of two contiguous vertebral bodies with considerable endplate sclerosis, findings characteristic of discitis.
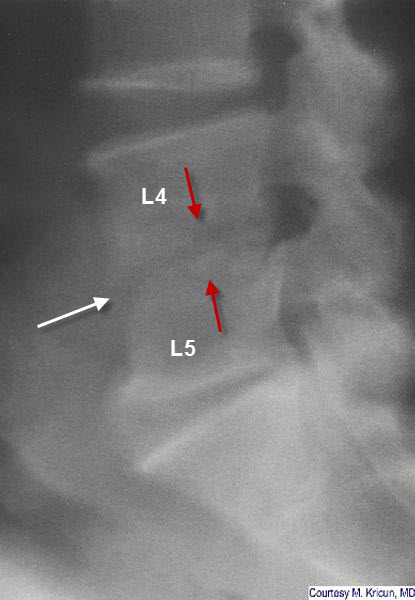
Discitis, Lumbar Spine. There is destruction of the normal endplates
(red arrows) of L4 and L5 with narrowing of the intervening disc space.
Radiologic Clinics, Imaging of the Spine, 1991
The Requisites, Neuroradiology
|
|
|
