|
|
Esophageal Atresia and Tracheo-esophageal Fisula
TEF
General Considerations
- Etiology not completely understood
- Faulty separation of primitive trachea and esophagus most widely accepted
- Esophageal atresia with fistulous connection to the distal pouch is more common than esophageal atresia alone or tracheoesophageal fistula without esophageal atresia ( H-type fistula)
- Increased incidence of TEF with Down Syndrome
- About 30% of infants with esophageal atresia/tracheoesophageal fistula are born prematurely
- Esophageal atresia commonly associated with other abnormalities of the GI tract including
- Imperforate anus
- Duodenal atresia or stenosis
- In 25% of cases, there are 13 or more pairs of ribs or 6 or more lumbar vertebral bodies
- VACTERL=vertebral, anal atresia, cardiac abnormalities, TEF and/or esophageal atresia, Renal agenesis and dysplasia and limb defects
Clinical findings
- Presentation for all types is typically early, except for H-type which may go undiagnosed until late childhood
- Symptoms include
- Choking
- Drooling
- Difficulty handling secretions
- Regurgitation
- Aspiration
- Respiratory distress
Imaging findings
- Depends on the type
- Prenatal ultrasound can suggest diagnosis as early as 24 because of polyhydramnios
- Aspiration pneumonia often involves the RUL when there is esophageal atresia
- Radiolucent, blind-end dilated pouch of upper esophagus may be seen on chest x-ray
- Confirmed on lateral view
- Anterior displacement of trachea
- Rarely, air-fluid level in pouch
- With esophageal atresia and no fistula, no air enters GI tract
- Abdomen is airless
- Stomach should have air in it 15 minutes after birth normally
- With a distal communication between esophagus and trachea, there is gas in abdomen
- Further imaging studies are usually not necessary but introduction of a soft catheter into the pouch will prove the diagnosis
- With H-type, pneumonia may be more widespread
- Only clue on lateral film my be close proximity of trachea and esophagus
- If barium is introduced through a tube for H-type fistula, it must start high in the esophagus as many fistulae are in the upper esophagus
- When seen, the H-type fistula characteristically slopes upward from the esophagus to the trachea
Treatment
- Primary anastomosis of proximal and distal esophagus usually when infant is a few months old
- Colonic interposition if primary anastomosis is impossible
Complications
- May have hypoplasia and stenosis of the distal esophagus
- Motility of distal esophagus may be impaired postoperatively (occurs in more than 90%)
- Also
- Fistulae and sinus tracts around surgical site
- Shortening of esophagus following repair may lead to hiatal hernia and reflux
- Focal tracheomalacia may occur from the distended upper esophageal pouch in utero
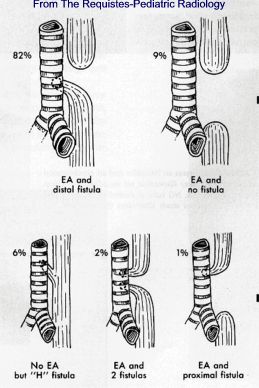
Types of esophageal atresia (EA) with/without
tracheoesophageal fistula
From The Requisites-Pediatric Radiology
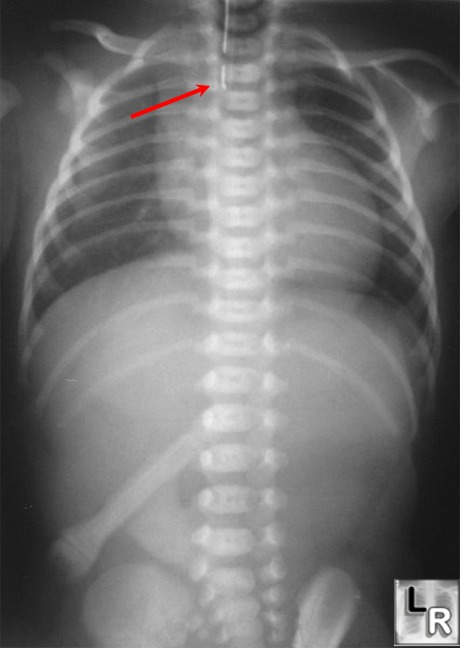
Esophageal Atresia. Red arrow points to end of orogastric tube which is
blocked from entering the distal esophagus
by the patient's esophageal atresia. Note the lack of gas in the abdomen
indicating a fistulous tract does not connect the trachea to the distal
esophagus.
Swischuk, L. 14th ed: Imaging of the Newborn, Infant and Young Child
Blickman, H. The Requisites: Pediatric Radiology, 2nd ed, 1998
|
|
|
