|
|
Complications of Endotracheal Tubes (ETT)
General Considerations
- The tip of the endotracheal tube should be about 5 cm from carina or roughly halfway between the clavicles and the carina
- This is because the tip may travel up to 2 cm downward if the neck is flexed or 2 cm upward if the neck is extended
Imaging Findings – Correct Position
- The carina is normally at the level of T5-T7
- Tip of tube is usually diagonally shaped with a marker stripe in the side of the tube
- 5 cm from carina
- Width of tube should be ½ to 2/3 width of trachea
- Cuff, if present, should not be inflated so as to distended the walls of the trachea
Imaging Findings – Malposition
- Most often malpositioned in right mainstem bronchus because of shallower angle right main bronchus makes with trachea than does left mainstem bronchus
- Right mainstem bronchus intubation will lead to atelectasis of entire left lung and hyperinflation right lung
- Bronchus intermedius intubation may lead to atelectasis of entire left lung and the right upper lobe
- ETT tip in the neck may lead to vocal cord injury
- Also may lead to perforation of the pyriform sinus, larynx or trachea and pneumomediastinum, subcutaneous emphysema, pneumothorax
- Esophageal intubation may be suspected if tube deviates from the tracheal air shadow and there is a dilated esophagus and stomach
Other Complications
- Aspiration/pneumonia
- Dependent portions of lungs
- Lower lobes
- Foreign body aspiration
- Broken teeth
- Dentures
- Fillings
- Pneumothorax, pulmonary interstitial emphysema, pneumomediastinum from barotrauma
- Rupture of alveoli from high pressures with mechanical ventilation
- Sinusitis from prolonged nasotracheal intubation
Long-term Sequelae
- More common with tracheostomy tubes than endotracheal tubes
- Laryngeal injury from scarring of posterior glottis, fusion posterior commissure, arytenoid injury, subglottic stenosis
- Tracheal stenosis
- Tracheomalacia
- Fistulae to esophagus, adjacent blood vessels
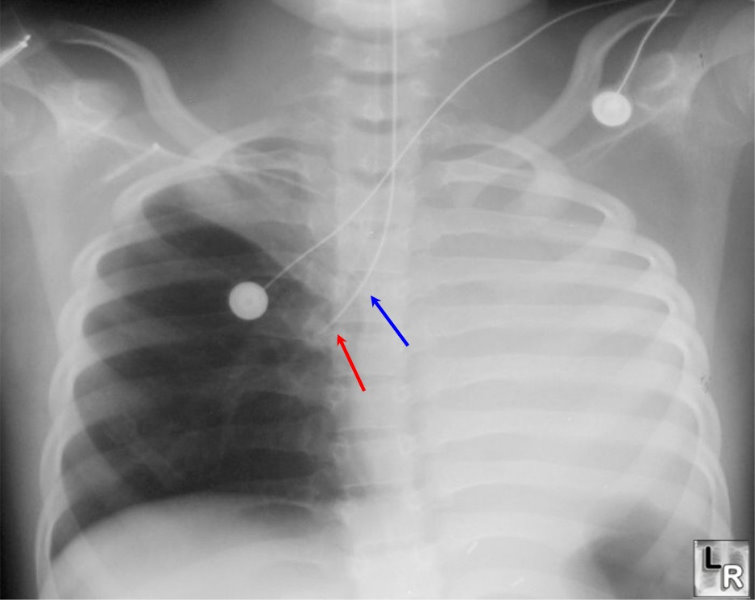
Atelectasis, Left Lung. Tip of endotracheal tube (red arrow) projects
below the carina
(blue arrow) into the bronchus intermedius on the right.
Goodman, L and Putman, C: Intensive
Care Radiology: Imaging of the Critically Ill W.B. Saunders, 1983
McCloud T: Thoracic Radiology: The
Requisites Mosby, 1998.
|
|
|
