|
|
Gastric Volvulus
- Uncommon
- May occur in children due to congenital
diaphragmatic defects
- In adults, rarely occurs before age 50
- Most common cause of gastric volvulus in
adults are diaphragmatic defects
- Stomach twists on itself
- Etiologies
- Abnormality of the suspensory ligaments of the
stomach
- Gastrohepatic
- Gastrosplenic
- Gastrocolic
- Gastrophrenic
- Unusually long gastrocolic and gastrohepatic
mesentery
- Classified as one of two types--organoaxial or
mesenteroaxial
Type |
Appearance |
Description |
Remarks |
Organoaxial |
 |
Twist occurs
along a line connecting the cardia and the pylorus--the luminal
(long) axis of the stomach |
· Most common type.
· Usually associated with diaphragmatic defects.
· Vascular compromise more common. |
Mesenteroaxial |
 |
Twist occurs
around a plane perpendicular to the luminal (long) axis of the
stomach from lesser to greater curvature |
· Chronic symptoms more common.
· Diaphragmatic defects less common. |
- Almost always occur with large diaphragmatic
hernia like hiatal hernia
- Especially, paraesophageal hiatal hernias
- In paraesophageal hernias, gastroesophageal
junction remains in abdomen while stomach ascends adjacent to the
esophagus
- Produces “upside-down-stomach”
- Gastric volvulus is most common complication
of paraesophageal hernias
- Also occurs with eventration of the diaphragm
- Paralysis of diaphragm
- Despite abnormal placement of stomach, it usually
does not become obstructed
- Sometimes called “partial volvulus” or “torsion”
or “chronic volvulus”
- Twisting up to 180 degrees may cause no
obstruction
- Twisting beyond 180 degrees almost always
produces obstruction
- Clinical findings
- Unless acute, patients are frequently
asymptomatic
- When acute and obstructing
- Abdominal pain
- Attempts to vomit without results
- Inability to pass an NG tube
- Together, these three findings comprise the Borchardt triad which is diagnostic
of
acute volvulus
- Reportedly occurs in 70% of cases
- Imaging findings
- Massively dilated stomach in LUQ possibly
extending into chest
- Inability of barium to pass into stomach (when
obstructed)
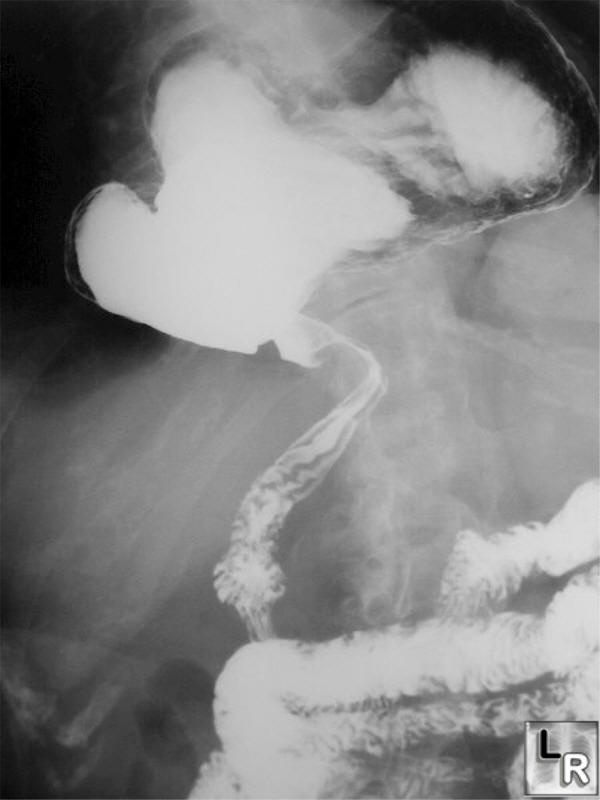
Gastric Volvulus. Frontal radiograph from an upper GI examination shows
the stomach
located in the lower chest in a large hiatal hernia. The greater curvature
of the stomach lies superior to the lesser curvature in an organoaxial
twist.
Note that the stomach is not obstructed.
- Treatment
- Surgery in acute gastric volvulus
- In patients with chronic gastric volvulus,
surgery is performed to prevent complications
- Nonoperative mortality rate = as high as 80%
- Mortality rate from acute gastric volvulus =
15-20%
- Mortality rate from chronic gastric volvulus
ranges up to 13%
- Complications
- Gastric emphysema
- Twisting of stomach may tear spleen from its
normal attachments
- Perforation is rare
- Margulis and Burhenne-Alimentary Tract Roentgenology
2nd Ed, Vol. 1
- Dahnert 4th edition
- eMedicine Gastric Volvulus by Mohamed Akoad, MD and
Richard Golub, MD
|
|
|
