|
|
Free Intraperitoneal Air
Pneumoperitoneum
- Etiology
- Disruption of wall of hollow viscus
- Blunt or penetrating trauma
- Perforating foreign body (eg,
thermometer injury to rectum)
- Iatrogenic perforation
- Laparoscopy / laparotomy (58%)
- Absorbed in 1-24 days depending on
initial amount of air introduced and body habitus (80% in
asthenic, 25% in obese patients)
- Leaking surgical anastomosis
- Endoscopic perforation
- Enema tip injury
- Diagnostic pneumoperitoneum
- Diseases of GI tract
- Perforated gastric / duodenal ulcer
- Perforated appendix
- Ingested foreign-body perforation
- Diverticulitis (ruptured Meckel
diverticulum / sigmoid diverticulum, jejunal
diverticulosis)
- Necrotizing enterocolitis with
perforation
- Inflammatory bowel disease (eg,
toxic megacolon)
- Obstruction* (gas traversing intact
mucosa): neoplasm, imperforate anus, Hirschsprung disease, meconium ileus
- Ruptured pneumatosis cystoides
intestinalis
- Idiopathic gastric perforation =
spontaneous perforation in premature infants (congenital
gastric muscular wall defect)
- Through peritoneal surface
- Transperitoneal manipulation
- Abdominal needle biopsy / catheter
placement
- Mistaken thoracentesis / chest tube
placement
- Endoscopic biopsy
- Extension from chest
- Dissection from pneumomediastinum
(positive pressure breathing, rupture of bulla / bleb, chest
surgery)
- Bronchopleural fistula
- Rupture of urinary bladder
- Penetrating abdominal injury
- Through female genital tract
- Iatrogenic
- Perforation of uterus / vagina
- Culdocentesis
- Rubin test = tubal patency test
- Pelvic examination
- Spontaneous
- Intercourse, orogenital insufflation
- Knee-chest exercise, water skiing,
horseback riding
- Intraperitoneal
- Gas forming peritonitis
- Rupture of abscess
- Air in lesser peritoneal sac gas in
scrotum (through open processus vaginalis)
- Imaging findings
- Large collection of gas
- Abdominal distension, no gastric
air-fluid level
- "Football sign" = large pneumoperitoneum
outlining entire abdominal cavity
- "Double wall sign" = "Rigler sign" = air
on both sides of bowel as intraluminal gas and free air
outside (usually requires >1,000 mL of free intraperitoneal gas + intraperitoneal fluid)
- "Telltale triangle sign" = triangular
air pocket between 3 loops of bowel
- Depiction of diaphragmatic muscle slips
= two or three 6-13 cm long and 8-10 mm wide arcuate
soft-tissue bands directed vertically inferiorly + arching
parallel to diaphragmatic dome superiorly outline of ligaments
of anterior inferior abdominal wall:
- "Inverted V sign" = outline of both
lateral umbilical ligaments (containing inferior epigastric
vessels)
- Outline of medial umbilical ligaments
(obliterated umbilical arteries)
- "Urachus sign" = outline of middle
umbilical ligament
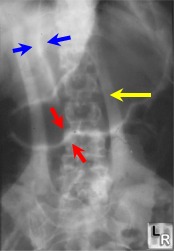
Blue arrows point to falciform
ligament, made visible by a large amount of free air in the peritoneal
cavity.
The red arrows demonstrate both sides of the wall of the stomach (Rigler's
sign), a sign of free air. The yellow arrow points to a skin fold.
- RUQ gas (best place to look for small
collections)
- Single large area of hyperlucency over
the liver
- Oblique linear area of hyperlucency
outlining the posteroinferior margin of liver
- Doge's cap sign = triangular collection
of gas in Morrison pouch (posterior hepatorenal space)
- Outline of falciform ligament = long
vertical line to the right of midline extending from
ligamentum teres notch to umbilicus; most common structure
outlined
- Lligamentum teres notch = inverted V-shaped area of hyperlucency along
undersurface of liver
- Ligamentum teres sign = air outlining
fissure of ligamentum teres hepatis (= posterior free edge of
falciform ligament) seen as vertically oriented sharply
defined slitlike / oval area of
hyperlucency between 10th and 12th rib within 2.5-4.0 cm of
right vertebral border 2-7 mm wide and 6-20 mm long
- "Saddlebag / mustache / cupola sign" =
gas trapped below central tendon of diaphragm
- Parahepatic air = gas bubble lateral to right edge of liver
|
|
|
