|
|
Esophageal Candidiasis
Monilial Esophagitis
- Most common cause of infectious
esophagitis
- Organism
- C. albicans
- Found in diseased skin, GI tract, female
genital tract, urine in patients with an with an indwelling
Foley catheter
- Usually occurs as an opportunistic
infection in those with
- Depressed immunity
- AIDS
- Hematologic disease
- Renal transplant
- Leukemia
- Chronic debilitating disease
- Diabetes mellitus
- Steroids
- Chemotherapy
- Radiotherapy
- Diseases which cause delayed esophageal
emptying
- Scleroderma
- Strictures
- Achalasia
- S/P fundoplication
- Rarely may occur in otherwise healthy
individuals
- Produces whitish slightly raised plaques
- Clinical Findings
- Dysphagia
- Odynophagia
- Intense substernal pain
- Associated with oral thrush (oropharyngeal
moniliasis) in 20-80%
- Location
- Predilection for upper 1/2 of esophagus
- Involvement of long esophageal segments
- Imaging Findings
- Discrete plaque-like lesions
- Plaques line-up longitudinally =
grouping of tiny 1-2 mm nodular filling defects with linear
orientation
- Larger plaques may coalesce to produce
"cobblestone" appearance
- Further coalescence produces “shaggy”
contour (from coalescent plaques, pseudomembranes, erosions,
ulcerations, intramural hemorrhage) in fulminant candidiasis
- More fulminant form is more often
associated with AIDS
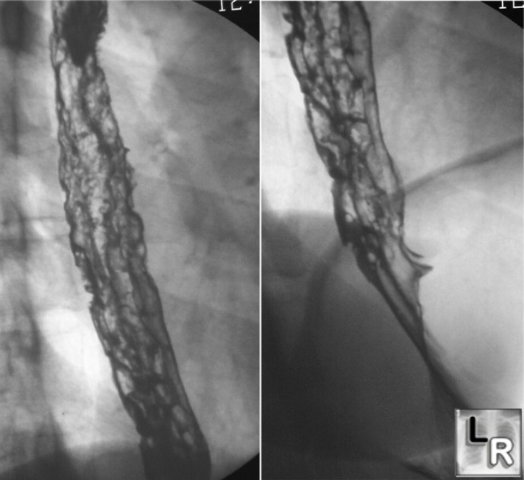
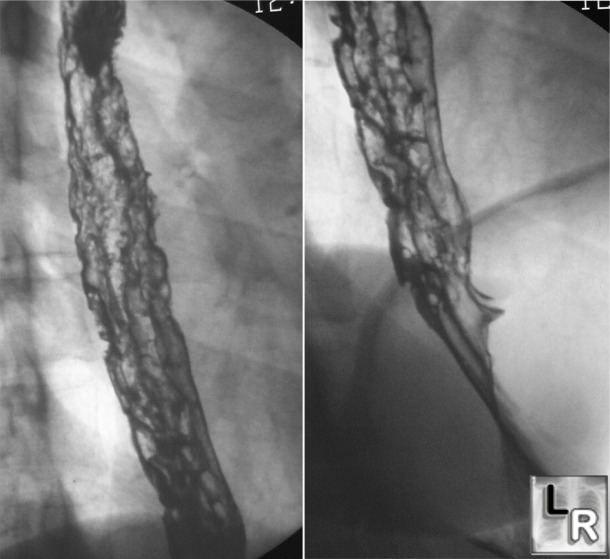
Candida Esophagitis (Moniliasis). Double-contrast esophagram shows markedly nodular
mucosa
with multiple discrete ulcers covering all of esophagus
- Ulcers invariably appear only on a background of diffuse plaque formation, not as isolated
findings
- Long, smoothly-tapering strictures may
develop but are rare
- More likely to develop in patients with
cutaneous manifestations of Candidiasis
- Mycetoma resembling large intraluminal tumor
is rare
- Diagnosis
- Endoscopy most sensitive method of making
diagnosis for mild cases
- Double-contrast esophagography should pick
up 90% of cases
- Treatment
- Mycostatin®
- Findings usually regress quickly
- Differential Diagnosis
- Glycogenic esophagitis – asymptomatic
nodularity
- Reflux esophagitis – distal esophagus,
nodules poorly defined
- Superficial spreading carcinoma- nodular
and irregular folds
- Artifacts (undissolved effervescent
crystals, air bubbles, retained food particles)
- Herpes esophagitis – discrete ulcers
surrounded by halo of edema
- Acute caustic ingestion – long strictures
are common
- Intramural pseudodiverticulosis – unlike
ulcers, pseudodiverticula don’t appear to connect to lumen
- Varices – distal esophagus usually;
serpiginous elongated filling defects

Candidiasis. Multiple images from a barium esophagram show slight irregularity of the wall (red arrows) caused by shallow ulcerations and deeper, barium-containing ulcers as well (white oval).
|
|
|