|
|
Eventration of the Diaphragm
General Considerations
- Congenitally thin muscular portion of the hemidiaphragm
- Appears to increase with age
- Usually occurs anteromedially and on the right with a right to left ratio of 5:1
- When on left, it frequently involves the whole hemidiaphragm
- May contain liver or sometimes kidney on right
Clinical Findings
Imaging Findings
- Smoothly marginated soft tissue density contiguous with the hemidiaphragm
- Appearance is characteristic
Treatment
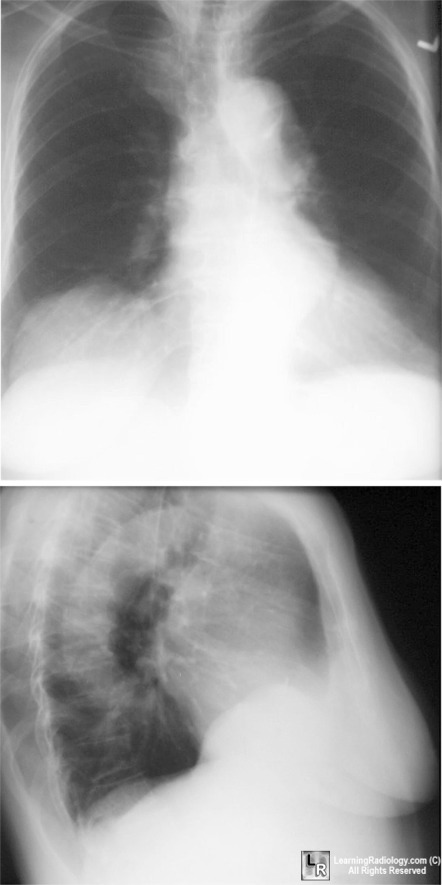
Eventration of the Diaphragm. Frontal and lateral chest x-ray shows smooth elevation
of right hemidiaphragm
medially and anteriorly consistent with an eventration of the hemidiaphragm
|
|
|
