|
Post-Pneumonectomy Changes
Broncho-Pleural Fistula
- First 24 hours, postpneumonectomy side contains only
air
- Slight shift of the mediastinum toward the
pneumonectomized side
- Slight elevation of ipsilateral hemidiaphragm
- Postpneumonectomy space fills with serosanguinous
fluid at rate of 2 rib spaces/day
- By end of 2 weeks, 80-90% of space obliterated
- By 4 months, complete obliteration
- Mediastinum gradually shifts more toward side of
pneumonectomy
- Maximum shift at 6-8 months
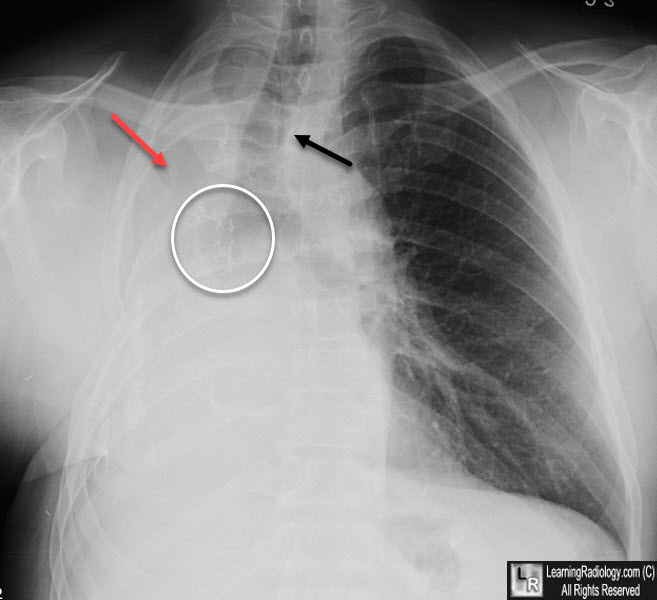
Post-pneumonectomy. There is complete opacification of the right hemithorax. There is a shift of the heart and mediastinal structures, such as the trachea (black arrow) towards the right indication volume loss. The right 5th rib is surgically absent (red arrow) from the surgery. There are multiple surgical clips seen adjacent to the stump of the right main bronchus (white circle).
- Failure of this ipsilateral shift almost always
indicates an abnormality in the postpneumonectomy space, including:
- BP fistula
- Empyema
- Hemorrhage
- Chylothorax
- Pneumonectomized side fills more rapidly on the left
than the right and more rapidly when the pneumonectomy is extrapleural
(i.e. includes the parietal pleura)
- Most sensitive indicator of late complications is
the return to midline of a previously shifted mediastinum
- Causes
- Recurrent neoplasm
- BP fistula
- Hemorrhage
- Chylothorax
- Empyema
- Rare complications
- Herniation of the heart through a pericardial
defect after radical pneumonectomy with a partial pericardiectomy
- Post-pneumonectomy syndrome
- More on right side
- More in children and adolescents
- Produces marked rightward and posterior
displacement of the mediastinum
- This, in turn, produces clockwise rotation of
the heart and great vessels
- Trachea and left main bronchus are compressed
between the aorta and pulmonary artery
- Leads to dyspnea and recurrent left-sided
pneumonia
- Displacement of the overinflated left lung into
the anterior right hemithorax
· Broncho-pleural fistula
o Incidence 2%
o Mortality 30-70%
o Causes:
§ Necrosis of bronchial stump
§ Dehiscence of suture line
o More common on the right
o Increased risk in association with
§ Residual carcinoma
§ Preoperative radiation
§ Diabetes
o Clinical
§ Sudden onset of dyspnea
§ Expectoration of bloody fluid
o Imaging findings
§ Return to midline of a previously shifted mediastinum
§ A drop in the fluid level by more than 2 cm is abnormal
§ Thin-section CT may demonstrate the BP fistula
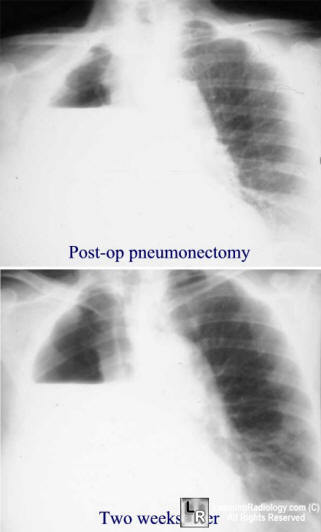
Bronchopleural Fistula. Top image demonstrates an air-fluid level normal for the 5th
post-operative day;
the lower image taken two weeks later shows a drop in the
height of the fluid level highly suggestive of a bronchopleural fistula
Fraser and Pare
|
